
Basics principles of functional stereotactic surgery
Thanks to anatomical and neurophysiological studies conducted over the past 100 years, the brain sections for planning and execution of movements and processing of perceptions such as seeing, hearing, touch, smell, and the pain are known. These are located in well-defined portions of the brain mantle (cortex) and in low-lying small switching cores, which are connected by paths with the appropriate areas of the cortex or the spinal cord. The idea of functional stereotactic is to selectively disable certain small switching cores or connecting tracks, and thereby influence - within a very small space and with low injury - very effectively the movements or the pain processing. The position of these switching cores and webs is known from specific anatomical atlases and can be determined in magnetic resonance images of the patient. Since the structures which have to reached are very small, ranging from the size of a bean to a rice grain, a very accurate calculation and mechanically extremely precise insertion of the probe to the desired destination point is necessary. Great importance is also attached to the intraoperative control. This is done by repeated verification of the electrode position in X-ray images, also by registering the cell discharge with microelectrodes and by observing the irritation caused by electrical stimulation of the microelectrode tip. The stereotactic method was developed 70 years ago for the treatment of functional disorders and applied successfully worldwide in the meantime on more than 100 000 patients. Originally a small lesion was set at the target point. For about 20 years non-destructive and reversible stimulation methods are preferred with implanted electrodes, due to fewer side effects. Because the target points for the lesion and for stimulation are the same, it must be assumed that the stimulation suppresses the activity or transmission of the pulses during the irritation. The calculation has since evolved from invasive methods with puncture and contrast filling of the ventricles towards noninvasive CT / MR procedures on computer design stations.
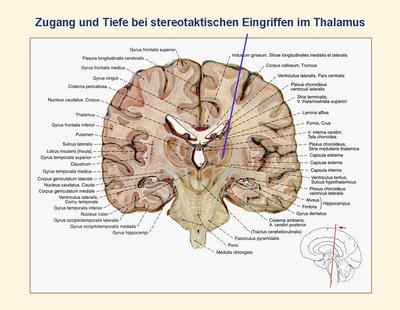
Fig.7
The target structures depend on the type of disease. An important target for the treatment of pure trembling (tremor) is the VIM nucleus (nucleus is. ventral intermediate) of the thalamus. The blue line in Figure 7 shows the access and the tip of the target point in the VIM nucleus of the thalamus in a frontal brain slice. If in case of Parkinson's disease in addition to the tremor and rigidity (rigor), uncontrolled movements (dyskinesia) or disabilities (akinesia) are occurring, then all these symptoms are most effectively deactivated through a small core between the thalamus and the midbrain, the so-called STN (subthalamic nucleus).
These operations require close coordination and cooperation with the Department of Neurology. This applies to the selection of suitable candidates, the neurological and electrophysiological testing during surgery and follow-up with change of drugs and fine adjustment of stimulation parameters. This is ensured by regular weekly meetings of neurosurgeons and neurologists treated at Saarland University Medical Center.
Contact Stereotaxis
Neurosurgical Team:
OÄ Dr. med. Dörthe Keiner
Phone: 06841-1614450
Email:Doerthe.Keiner @uks.eu
Prof. Dr. med. Peter Grunert
Phone: 06841/16 24451 oder 06841/16 24100
Email:Peter.Grunert @uks.eu
Registration for Admission:
Sr. Susanne Mathieu
Phone: 06841/16 24421
Neurological Team:
Prof. U. Dillmann, PD J. Spiegel, OA J. Bürmann
available via ambulance for Parkinson´s disease
Phone: 06841/16 24138
or EMG 06841/16 24116

