
Selective Internal Radiotherapy (SIRT) - Radioembolisation
SIRT is a modern and effective form of treatment for liver tumors or metastases that can no longer be treated surgically. SIRT is performed jointly by a nuclear medicine physician and a radiologist.
How is the SIRT carried out?
Under screening, a catheter is positioned via the groin near the tumor in the hepatic artery; a radioactive substance is administered, after its binding either to tissue-compatible resin spheres (SIR-Spheres®) or to glass spheres (Thera-Spheres®), directly into the tumor-supplying vessels. The spheres have a small diameter of about 20-40 µm and clog in the finest vessels that supply the tumor. The radioactive substance with which the spheres are marked is called Yttrium-90 (Y-90) and has optimal features for this treatment. It emits high-energy ß-radiation, which achieves a very high radiation dose in the tumor with protection of the healthy liver tissue surrounding the tumor and other nearby organs by providing a small range of <1 cm in the tissue. A 48-hour in-patient admission at a specially equipped ward of the Nuclear Medicine Clinic is required after treatment.
Who provides the indication for SIRT?
The indication for SIRT is made jointly by treating oncolocists, nuclear medicine physicians and radiologists.
What preparation is required for SIRT?
The possibility of SIRT treatment is assessed on a professional medical level. In addition, patients are informed about the treatment on a detailed preliminary consultation and an indispensable preliminary stationary examination is carried out.
The preparation procedure for the SIRT includes the following items:
- Detailed anamnesis about the disease and the previous treatment Current laboratory (liver function parameters, blood count, tumor markers).
- Magnetic resonance imaging / computer tomography of the liver.
- Positron emission tomography (PET) to exclude further metastases outside the liver.
- Diagnostic angiography (vascular imaging of the hepatic arteries) showing the appropriate location for an occlusion of laxative vessels.
- Injection of a low-level radioactive test substance (99mTc-MAA) followed by planar scintigraphy to check the extent of angiographic vascular occlusion and a possible shunt.
Case Report II SIRT
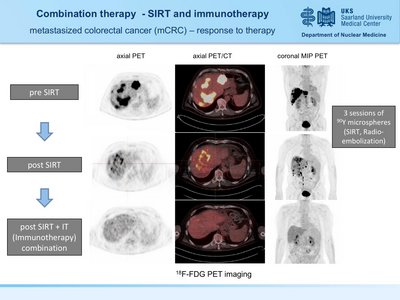
60y old male patient with hepatic metastasized rectal carcinoma. Patient had hepatic progression after two lines of chemotherapy and recieved three treatment cycles of selective internal radiotherapy (SIRT) followed by immunotherapy. The heavy tumor burden was dramatically reduced by SIRT with a complete remission after immunotherapy. No hematological toxicity was noted and quality of life was significantly improved. Therapy monitoring was performed by PET using 18F-FDG.
Are there contraindications to SIRT?
There are relative and absolute contraindications, which may differ depending on the chosen radioactive preparation for treatment:
Relative:
- Detection of small metastases outside the liver
- Volume of the collateral circulation (shunt volume) between liver and lungs 10 to 20%
- Partial sealing of the portal vein
Absolute:
- Larger tumor metastases outside the liver
- significantly reduced liver function and/or detection of abdominal fluid collection (ascites)
- Volume of the collateral circulation (shunt volume) between liver and lungs >20%.
- complete sealing of the portal vein

What complications or side effects of SIRT are known?
- Complications during and after SIRT are rare. A major complication is the possibility of placement of radioactive spheres outside the liver, e.g. in the stomach or intestinal wall. This can lead to inflammation of the gastric mucosa or even to an ulcer.
- In case of a collateral circulation (shunt) between the liver and lungs, a radiation-induced pneumonia can occur. However the presence of a collateral circulation is assessed using the test substance before the SIRT is carried out.
- Allergic reactions to the spheres have not yet been described.
How does the SIRT work?
The SIRT comprises the following steps:
- Indication testing by the attending physicians
- Detailed clarification discussion
- Carrying out preparatory examinations and, if necessary, radiological intervention on liver or tumor vessels (see above)
- Stationary admission and execution of a new vascular imaging of the hepatic arteries (angiography), followed by insertion of the yttrium-loaded spheres
- Control of the distribution of spheres by means of a scintigraphy
- 48-hour in-patient admission at a specially equipped ward
Is follow-up necessary after SIRT?
Follow-up is of great importance after the application of an SIRT. It is carried out in cooperation with the referring physicians from the gastroenterology clinic. It includes regular laboratory controls (liver function) as well as CT/MRI controls to assess the success of the therapy.
How often is the SIRT repeated?
SIRT is usually performed as a single one-day treatment, in individual cases, it may be repeated if liver disease recur.

