
Meningiomas
General Information
Meningiomas develop from “arachnoid cap cells” and are therefore strictly speaking no brain tumors. They are usually slow-growing and thereby crowd out the actual brain tissue. These tumors can also occur in the spinal canal or in the eye socket (orbit). In particular, in functionally less important areas of the brain, these tumors can often reach impressive sizes. In contrast, small tumors can already cause discomfort in critical regions. Regarding the total number of brain tumors meningiomas make up to 15% of diseases in men and 30 % in women and they occur mostly between the ages of 50 and 60 years. They affect women generally somewhat more frequently and at an older age. Typical locations are the falx (midline), the convexity of the sphenoid, the olfactory groove or the cerebellopontine angle.
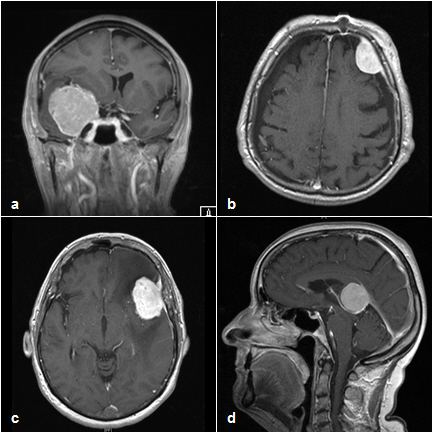
Depiction of different localized meningiomas on the MRI with contrast agents: high front on the left (a), sphenoid wing on the left (b) and on the right (c) and tentorium (d)
Classification
Meningiomas are classified according to the World Health Organization (WHO) grading system into three grades, based primarily upon the growth rate and the likelihood of recurrence - even after complete removal.
- WHO ° I (about 85%): slow growing, benign, recurrence after complete removal unlikely
- WHO ° II (8-10%): atypical, meningiomas with a tendency for recurrence
- WHO ° III (about 2-5%): anaplastic, fast growing meningiomas with clear signs of malignancy
Symptoms depend largely on the location of the tumors and which parts of the brain exert pressure on them. Intracranial pressure (e.g. headache, fatigue, nausea, and dizziness), neurological deficits (for example paralysis, impaired vision, gait, speech disorders) or epileptic seizures can occur. In many cases, however, a meningioma also triggers no symptoms and is discovered only by chance.
The diagnosis is made by CT and MRI's imaging. These images can also be used during surgery for neuronavigation to accurately localize the tumor and surrounding brain structures. Depending on the findings, other examinations such as angiography may be required.
The treatment of choice is the complete surgical removal of the meningioma. This is done by using microsurgical techniques and generally using neuronavigation and different techniques of intraoperative monitoring. In case of tumors, which are particularly rich in blood vessels, in certain cases of embolization (occlusion) of tumor vessels may be necessary to avoid intraoperative excessive bleeding. A subsequent radiation therapy is recommended for anaplastic meningiomas and can be an option in the case of incomplete resection of atypical meningiomas.
Our Expertise
- Complete spectrum of meningioma treatment
- Neurooncological research
Medical Contact Person
OA PD Dr. med. R. Ketter
Email: Ralf.Ketter @uks.eu
HSA-Consultation Hours:
Tuesday 9am-2pm
Registration
HSA-Consultation Hours:
Tel.: 06841-1624412

